




Contents
Scroll to:
https://doi.org/10.29326/2304-196X-2025-14-1-24-31
Scroll to:
Introduction. Lumpy skin disease (LSD) is currently a matter of veterinary concern due to the significant economic losses of the live stock in dustry. The risk of LSD spread and penetration into the disease-free countries is increasing every year. Therefore, timely monitoring of the infection spread for the development a strategy for this disease control becomes of current importance. Description of thedisease manifestations and course, evaluation of historical and statistical data on LSD spread in the Middle Eastern countries as well as the further joint actions at the international level are presented in this review.
Objective. Analysis of historical and statistical data on clinical lumpy skin disease in the Middle Eastern countries.
Materials and methods. The following electronic databases were used for relevant data searching and collection: PubMed, Web of Science, eLIBRARY.RU, mdpi.com, frontiersin.org, researchgate.net, etc. English literature data for 10 years were analyzed.
Results. In 1988 LSD spread outside the African continent then LSD stayed for a short time within the MiddleEastern countries and two years later spread further to the west and east. Despite the further spread, recurrent LSD outbreaks were reported in the Middle Eastern countries over the next few years. Many countries in the Middle East still face the problem of uncontrolled livestock movement, lack of high-quality laboratory diagnostics, and irregular contacts with international health and surveillance organizations aggravated by the unstable political situation in the region. These problems indicate the importance of LSD control at the international level, the significance of regional and international cooperation and effective biosafety policies.
Conclusion. Role of the Middle East region in LSD virus spread, probable causes of LSD infection in the region, trends for further actions for LSD control were determined.
Khatib Ya. Lumpy skin disease in the Middle East – historical and statistical data. Veterinary Science Today. 2025;14(1):24-31. https://doi.org/10.29326/2304-196X-2025-14-1-24-31
Lumpy skin disease is currently a matter of veterinary concern due to the significant economic losses to the livestock industry caused by this disease. Lumpy skin disease is caused by a DNA virus genus Capripoxvirus, family Poxviridae, and affects cattle and water buffaloes and characterized by skin nodules in infected animals. This virus is antigenically closely related to sheep poxvirus and goat poxvirus, therefore it can infect small ruminants without any clinical disease manifestations [1][2][3].
The disease is enzootic, rapidly explorative and sometimes fatal infection, despite the fact that, as often reported, LSD is characterized by high incidence rate (more often about 20%, but it can vary from 3 to 85%) and rather low mortality rate (less than 5%) [4][5][6][7]. LSD affects food-producing animals that results in reduced milk yields in dairy animals and decreased weight gains in meat animals that has a negative effect on food security due to limited availability of high-quality animal products on the world market. Reproductive performance in infected animals as well as quality of hides derived from slaughtered animals significantly reduce [2][5][6][8][9][10]. In addition, the disease affects trade links and requires financial costs for anti-epizootic measures. Taking into account its ability to spread rapidly across the borders of countries and cause significant damage, the World Organization for Animal Health has included LSD in the list of the most economically significant and notifiable transboundary viral animal diseases.
Lumpy skin disease was first reported in 1929 in Northern Rhodesia (now Zambia) and since that time the disease outbreaks have occurred in various parts of Africa. But the disease was contained to the African continent. In 1988–1989 the disease cases were registered in Egypt and Israel, and then LSD began to progressively spread to the countries of the Middle East, Eastern Europe, Russia and the Balkan Peninsula [4][11][12].
In 2019 LSD has already been reported in South and East Asia. This has put livestock industry at risk in such countries as Afghanistan, Pakistan, India, etc. LSD is also detected in cattle in China, Cambodia, Singapore, and Indonesia, and there is a threat of LSD spreading to the LSD-free countries with significant livestock populations (Australia, etc.) [4][6]. There are also the first reports LSD in humans [10], although, according to other data, the virus is not transmitted to humans [2].
The risk of further LSD spread and penetration into the disease-free countries is increasing every year. Therefore, timely monitoring of the infection spread for the development a strategy for this disease control becomes of current importance.
Description of the disease manifestations and course, evaluation of historical and statistical data on LSD spread in the Middle Eastern countries as well as the further joint actions at the international level are presented in this review.
The work was aimed at analysis of historical and statistical data on clinical lumpy skin disease in the Middle Eastern countries.
English literature data on LSD in the Middle East for the last 10 years were analysed. The following electronic databases were used for relevant data searching and collection: PubMed, Web of Science, eLIBRARY.RU, mdpi.com, frontiersin.org, researchgate.net, etc.
Lumpy skin disease is transmitted by biting insects. The virus is transmitted by blood-sucking mosquitoes (Aedes aegypti), biting flies (Stomoxys calcitrans, Haematobia irritans, Musca domestica) and some tick species (Rhipicephalus appendiculatus, Rhipicephalus decoratus, Amblyomma hebraeum) [13]. LSD can also be transmitted by non-vector route, through contact of animals with fomites (feeders, waterers), through milk, semen, or in utero [6, 10]. Hot and humid climate, rainy seasons, and low-lying, swampy terrain are factors contributing to multiplication of LSD vectors [1][4][9].
Clinical LSD takes the following forms: acute to subclinical or chronic form. The main symptoms include fever, lack of appetite, oedema, generalized nodular skin lesions, enlarged lymph nodes, emaciation, decreased lactation and abortions in pregnant animals. Severe LSD form is characterized with ulcerative mucosal lesions in oral cavity, larynx, trachea and esophagus. LSD virus localized in the reproductive system can cause temporary or permanent infertility in cows and bulls [7][8][9].
The virus is excreted by various routes: via lachrymal and nasal secretions, blood, saliva, milk, and semen of the infected animals. Nodules appearing on the mucous membranes of the eyes, nose, mouth, rectum, udder and genitalia quickly and then ulcerating can be attributed to the priority routes of virus shedding [9].
Strict quarantine of animals entering the farm, control of disease vectors, and preventive livestock vaccination are the most important measures for LSD eradication and prevention. Measures for LSD control at the international level, regional and international cooperation, and an effective biosafety policy are also of great importance [14].
The first LSD case in Northern Rhodesia in 1929 was considered to be hypersensitive response of animals to insect bites and was designated by the term “pseudocranivaria”. The infectious nature of the disease was discovered in the period from 1943 to 1945, when LSD was already recorded in Southern Rhodesia (now Zimbabwe), Botswana and South Africa. By 1946, the disease had spread to Mozambique, in 1950 it was detected in Angola and Zaire, in 1954 – on Madagascar, in 1956 – in Namibia, Tanzania and Uganda. Over the next three decades, LSD were reported in different African countries (Kenya, Sudan, Chad, Niger, Ethiopia, etc.), and therefore the virus has long been considered endemic to African countries [4][10].
After the disease was reported in Egypt in 1988–1989, LSD spread outside the African continent and was detected in Israel. Earlier, in 1984, LSD outbreak was reported in Oman, but disease cases were not confirmed, although the disease cases were repeatedly reported in 2009. In 1986, LSD was detected in Kuwait, and the second LSD outbreak occurred in 1991. The disease was reported in Lebanon in 1993, in Yemen in 1995, in the UAE in 2000, in Bahrain in 1993 and again in 2002, and in Saudi Arabia and Iraq in 2013 [4][15].
In 2014 LSD outbreak was reported in Azerbaijan. In 2015 LSD was registered in such European countries as Greece, Albania and Russia (another extensive outbreak occurred in Russia in 2017). Large-scale vaccination against LSD was initiated in European countries for prevention of the wide spread of infection, but disease cases nevertheless occurred [16]. In 2016 and 2018 LSD was reported in Georgia, and in 2018 it was detected in such countries of the Balkan Peninsula as Greece, Bulgaria, North Macedonia, Serbia, Kosovo and Albania [4][17].
Figure 1 shows map of LSD outbreaks reported in 2013–2017 in the Middle East and neighbouring countries [18].
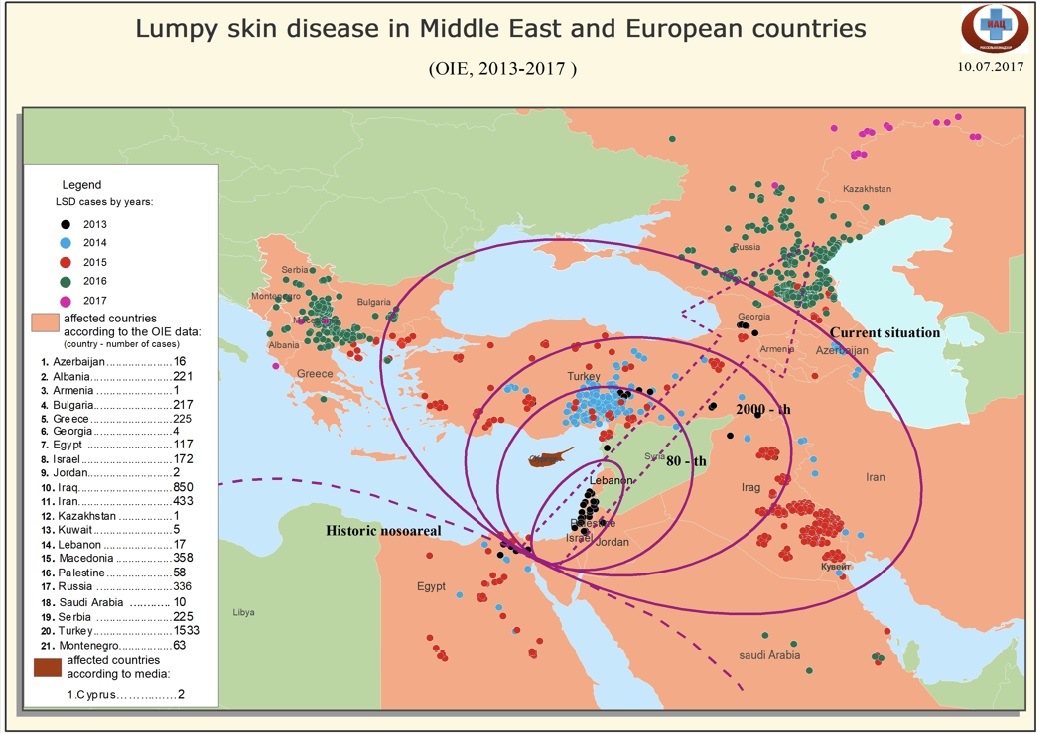
Fig. 1. LSD outbreaks reported from 2013 to 2017 in the Middle East region and neighboring countries [18]
Since 2019 LSD has become a serious problem for livestock industry in Asian countries. The disease caused devastating outbreaks in Bangladesh (2019–2020), then in India and China (2020), spread further to Nepal, Bhutan, Sri Lanka, Vietnam and Malaysia (2020). In 2021 LSD was reported in Thailand, Laos NDR, Pakistan and detected in Indonesia and Singapore in 2022 [4].
Morbidity and mortality reported during the Eurasian epizootics are approximately 10% and 1%, respectively, which, according to some authors, depends on the genetic predisposition of cattle to LSD.
As for Middle East region, LSD stayed for a short time within the region after spread outside the African continent and two years later spread further to the west and east. In the Middle East region, recurrent disease outbreaks were reported over the next few years. Some of them reported in the scientific literature are described below.
In 2012–2013, LSD virus was detected in Syria and Iraq. The unstable political situation, civil conflicts and wars had a negative impact on the veterinary services activities, contributing to the further pathogen spread to neighbouring countries of Southwest Asia [1][6]. No specific treatment of infected animals was performed, and conservative intervention was limited to symptomatic therapy [6].
In 2013, LSD was detected in Turkey near the borders to Syria and Iraq [19][20][21][22][23]. The infected animals were not vaccinated against the infection. Mass immunization of cattle had been started in Turkey since 2014, but outbreaks had been still recorded until 2019 [6][24].
In 2013 LSD was found in cattle in Jordan. Infected herds were treated with broad-spectrum antibiotics and anti-inflammatory drugs [6].
In 2014 LSD was still recorded in Iraq (9 disease outbreaks were reported in 2014) [9][25].
In 2014–2016, the disease outbreaks were reported in Iran, where the disease presumably spread from Iraq due to the uncontrolled movements of infected animals across the common border [26][27][28]. According to P. Sameea Yousefi et al. [7] 683 cattle were examined for LSD clinical signs (fever, lack of appetite, decreased milk yield, detection of typical skin nodules and enlarged lymph nodes) during two-year observation period and the above-mentioned signs were detected in 122 cattle (prevalence – 17.9%). Therewith, the highest disease incidence rate was observed in animals older than 5 years, and the lowest in animals younger than 6 months. In vaccinated cattle, clinical signs were observed in 40.8% of animals, in non-vaccinated cattle – in 71.3% of animals. At the disease prevalence of 17.9%, the total mortality and lethality in the four examined Iranian provinces were 3.5 and 19.7%, respectively, that was non-consistent with earlier data from Turkey (12.3% morbidity and 6.4% mortality) [29], Oman (13.6–29.7% morbidity and 15.4–26.3% mortality) [30], Jordan (26.0% morbidity and 1.9% mortality) [31], Saudi Arabia (6.0% morbidity and 0.99% mortality) [32]. This inconsistency of the data on the disease prevalence and mortality is explained by the authors of the above study by variability of factors contributing to LSD (climate humidity, ambient temperature, etc.).
In 2018 and 2019, outbreaks continued in Iraq, namely in Basra province. The overall disease prevalence in all age groups of cattle was 18.7% (112 infected animals were detected out of 600 examined animals). LSD was detected in 92.8% of diseased animals, arthritis in 17.8% of diseased animals, and lymphadenopathy was detected in 2.5% of diseased animals [8].
The organization and quality of animal movement control and specific LSD prevention in the Middle Eastern countries depend on the well-coordinated activities of veterinary services. Stamping out of infected animals carried out in Egypt and Israel enabled LSD eradication in these countries in 2006. However, other Middle Eastern countries still face the problem of uncontrolled livestock movements, lack of high-quality laboratory diagnostics, and irregular contacts with international organizations in the field of animal health and surveillance, exacerbated by the unstable political situation in the region [1].
Lumpy skin disease is a serious problem for livestock industry in many countries due to its rapid spread and resulting economic losses. The disease originated from African countries has gradually affected Middle Eastern and Asian countries and now threatens Western Europe and Australia. Joint efforts aimed at livestock movement control, reducing the risk factor, destruction of contaminated objects (dead animals and infected materials) are required for prevention of the further LSD spread and for LSD eradication in the countries already affected by this disease.
Currently, infection spread control is of particular importance due to the significant number of outbreaks reported in the Middle East, and risk of LSD transmission out of this region both to the west, towards the Balkan Peninsula and Europe [33], and to the east and southeast, towards Asian countries and further to Australia and New Zealand, having large cattle populations and remaining free from the disease. The further LSD spread could lead to significant economic losses in the global livestock sector.
Therefore, the Middle East can be considered as a port of entry for the infection spreading outside Africa to Europe and Asia. Thus, Figure 1 clearly shows the spread of the disease from Egypt and Israel to other countries in the Middle East, then westward to the Balkan Peninsula, northward to the southern regions of Russia, and eastward to Asian countries.
The rapid LSD virus spread in different countries can be accounted for cattle movements across international borders and for migration of blood-sucking insects regarded as disease vectors.
Figure 2 shows the directions of domestic ruminant movements in Africa and Middle East and links of livestock migration flows in these regions with Asian countries [34]. The map shows that the Middle East has close links with African and other Asian countries as for livestock purchase and sale. This significantly increases the risk of transmission of infectious large and small ruminant diseases through the territories of Middle Eastern countries to new territories.
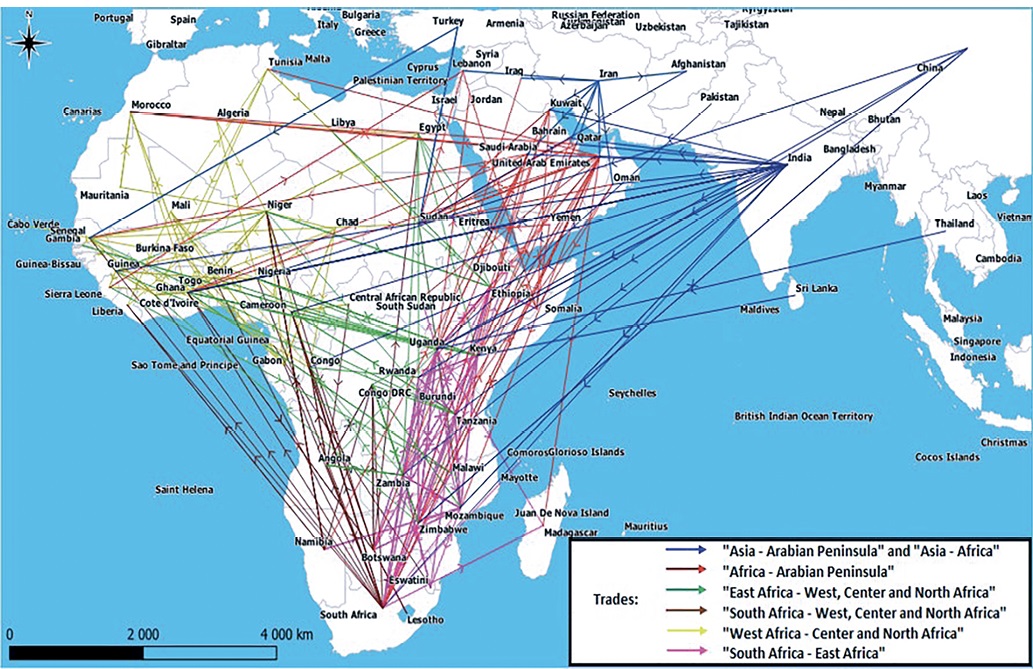
Fig. 2. Mapping of irregular flows of domestic ruminants in Africa and their links to Asia [34]
Time intervals of LSD appearance on each of the continents were examined.
Aggregated table on the reported disease outbreaks shows that since its first occurrence in Zambia, from 1929 to 1988, i.e. for 59 years, the disease had remained within the borders of the African continent, and therefore LSD was considered endemic to African countries. There is no information about the country from which LSD virus was introduced into the Middle East, in Egypt, in 1988, although there are data on its further spread: the virus was introduced from Egypt to Israel, and in the next year both of these countries became the port of the pathogen entry to the Mediterranean countries, as well as other Middle Eastern countries. That was the way of LSD virus spread from the African continent to the Middle Eastern countries and further to the western (Mediterranean countries) and eastern (South, East and Southeast Asian countries) regions [35].
Table
LSD outbreaks sequentially reported in different world regions
|
Year |
Country |
Virus origin |
Possible ways of further spreading |
Time of LSD virus staying within one region before further spreading |
|
1929 |
Zambia |
unclear |
neighbouring African countries |
59 years within the African continent |
|
1943 |
Botswana |
Zambia |
Zimbabwe and South Africa |
|
|
1944–1945 |
Zimbabwe, South Africa |
Zambia, Botswana |
Sudan and Ethiopia |
|
|
1946–1956 |
Mozambique, Angola, Madagascar, Tanzania, Uganda |
Zambia, Botswana |
Border countries where cattle was imported |
|
|
1957 |
Kenya |
unclear |
African countries – cattle importers |
|
|
1971 |
Sudan |
insufficient data |
insufficient data |
|
|
1973–1974 |
Chad, Niger, Nigeria |
Cameroon via Gongola State in Nigeria |
insufficient data |
|
|
1981–1983 |
Ethiopia |
Sudan |
insufficient data |
|
|
1983 |
Somalia |
insufficient data |
insufficient data |
|
|
1988–1989 |
Egypt |
African countries |
European countries and Israel |
2 years within the Middle East countries |
|
1989 |
Israel |
Egypt |
insufficient data |
|
|
1990–2010 |
Mediterranean countries |
Egypt, Israel |
All neighbouring countries |
20 years − spread to the Mediterranean countries |
|
2012–2014 |
Mediterranean countries |
Syria, Iraq |
Greece, Bulgaria |
6–7 years − Eurasian LSD epizootic (spread of the virus in the South Eastern European, Middle Eastern and Eurasian countries) |
|
2013 |
Turkey, Iran |
Syria, Iraq |
insufficient data |
|
|
2015–2017 |
Russia |
Turkey, Azerbaijan, Iran, Kazakhstan |
Northern regions of Europe |
|
|
Countries located in the Balkan Peninsula |
Turkey |
Central and South Asian countries |
||
|
2019 |
Bangladesh |
Perhaps neighbouring countries |
India, Myanmar |
5 years − spread in Southeast Asian Countries |
|
India |
Nepal, Bhutan |
|||
|
2019 |
China |
Kazakhstan, Russia |
Taiwan |
|
|
2020 |
Nepal |
India, China |
unknown |
|
|
Vietnam |
China |
unknown |
||
|
2021 |
Thailand |
unknown |
insufficient data |
|
|
Pakistan |
India |
not clear |
||
|
Mongolia |
Russia, China |
China, India |
||
|
Cambodia |
not clear |
not clear |
||
|
2022 |
Afghanistan |
unknown |
insufficient data |
|
|
Korea |
China, Nepal |
insufficient data |
||
|
Indonesia |
India |
Indonesia, threat to the northern regions of Australia |
||
|
2023 |
Libya |
unknown |
Tunisia and other Northwest African countries (Maghreb) |
It should be noted that LSD virus “stayed” in the Middle East for the short period before its further spread to the Balkan Peninsula and further to the east to other Asian countries. This can be accounted for historically highly intensive trade relations in this region, climate suitable for virus vectors and insufficient control by veterinary surveillance authorities.
Specific preventive vaccination is currently the only effective method for LSD outbreak prevention, therefore, mass vaccination appears to be an important component of the general disease control strategy. In addition to cattle vaccination, strict quarantine measures for incoming animals, as well as slaughter of the diseased animals are required for successful eradication of LSD. Veterinary supervisory authorities should ensure strict control over LSD susceptible animal movements between neighbouring countries. Thus, the disease control should be carried out in animal farming industry at all levels: from farm to international supervisory agencies.
1. Alkhamis M. A., VanderWaal K. Spatial and temporal epidemiology of lumpy skin disease in the Middle East, 2012–2015. Frontiers in Veterinary Science. 2016; 3:19. https://doi.org/10.3389/fvets.2016.00019
2. Krivonos R. A., Dzhailidi G. A., Mischenko A. V., Mischenko V. A., Chernykh O. Yu., Shevkoplyas V. N., et al. Problem of lumpy skin disease outbreak prevention and eradication. Veterinary Science Today. 2017; (1): 45–49. https://veterinary.arriah.ru/jour/article/view/287/288
3. Abdulqa H. Y., Rahman H. S., Dyary H. O., Othman H. H. Lumpy skin disease. Reproductive Immunology: Open Access. 2016; 1 (4):25. https://doi.org/10.21767/2476-1974.100025
4. Akther M., Akter S. H., Sarker S., Aleri J. W., Annandale H., Abraham S., Uddin J. M. Global burden of lumpy skin disease, outbreaks, and future challenges. Viruses. 2023; 15 (9):1861. https://doi.org/10.3390/v15091861
5. Amin D. M., Shehab G., Emran R., Hassanien R. T., Alagmy G. N., Ha- gag N. M., et al. Diagnosis of naturally occurring lumpy skin disease virus infection in cattle using virological, molecular, and immunohistopathological assays. Veterinary World. 2021; 14 (8): 2230–2237. https://doi.org/10.14202/vetworld.2021.2230-2237
6. Saltykov Yu. V., Kolosova A. A., Feodorova V. A. Update of lumpy skin disease: emergence in Asian part of Eurasia. Acta Veterinaria. 2022; 72 (3): 287–299. https://doi.org/10.2478/acve-2022-0023
7. Sameea Yousefi P., Mardani K., Dalir-Naghadeh B., Jalilzadeh-Amin G. Epidemiological study of lumpy skin disease outbreaks in North-western Iran. Transboundary and Emerging Diseases. 2017; 64 (6): 1782–1789. https://doi.org/10.1111/tbed.12565
8. Aldeewan A. B., Muhsen R. K. Clinical and serological study of lumpy skin disease in cattle in Basrah Provence. Kufa Journal for Veterinary Medical Sciences. 2019; 10 (1): 99–104. https://doi.org/10.36326/kjvs/2019/v10i13329
9. Al-Sabaawy H. B., Al-Hamdany E. K., Al-Sultan A. A., Rdam S. A. A high light on lumpy skin disease in Iraq and the Middle East: A review article. Journal of Applied Veterinary Sciences. 2020; 5 (2): 94–103. https://www.researchgate.net/publication/347910605
10. Pal M., Gutama K. P. Can lumpy skin disease be considered a zoonosis? American Journal of Infectious Diseases and Microbiology. 2023; 11 (1): 13–17. https://doi.org/10.12691/ajidm-11-1-3
11. Makarov V. V. Global epizoothology. Russian Veterinary Journal. 2019; (6): 26–35. https://doi.org/10.32416/2500-4379-2019-2019-6-26-35 (in Russ.)
12. Elhaig M. M., Selim A., Mahmoud M. Lumpy skin disease in cattle: Frequency of occurrence in a dairy farm and a preliminary assessment of its possible impact on Egyptian buffaloes. Onderstepoort Journal of Veterinary Research. 2017; 84 (1):a1393. https://doi.org/10.4102/ojvr.v84i1.1393
13. Moosa-Kazemi S. H., Asgarian T. S., Sedaghat M. M., Akbarian M. The mosquitoes (Diptera: Culicidae) and their medical and veterinary importance in an arid zone of Central Iran. Biomedical Journal of Scientific & Technical Research. 2021; 40 (3): 32283–32290. https://doi.org/10.26717/BJSTR.2021.40.006455
14. EFSA Panel on Animal Health and Welfare (AHAW). Scientific opinion on lumpy skin disease. EFSA Journal. 2015; 13 (1):3986. https://doi.org/10.2903/j.efsa.2015.3986
15. Al-Salihi K. A., Hassan I. Q. Lumpy skin disease in Iraq: Study of the disease emergence. Transboundary and Emerging Diseases. 2015; 62 (5): 457–462. https://doi.org/10.1111/tbed.12386
16. EFSA, Calistri P., De Clercq K., Gubbins S., Klement E., Stege- man A., et al. Lumpy skin disease epidemiological report IV: data collection and analysis. EFSA Journal. 2020; 18 (2):e6010. https://doi.org/10.2903/j.efsa.2020.6010
17. Turan N., Yilmaz A., Tekelioglu B. K., Yilmaz H. Lumpy skin disease: global and Turkish perspectives. Approaches in Poultry, Dairy & Veterinary Sciences. 2017; 1 (1): 11–15. https://doi.org/10.31031/APDV.2017.01.000504
18. Lumpy skin disease in the Middle Eastern countries and Europe in 2013–2017. https://fsvps.gov.ru/wpcontent/uploads/2023/06/dermatit_east.pdf (in Russ.)
19. Ince Ö. B., Çakir S., Dereli M. A. Risk analysis of lumpy skin disease in Turkey. Indian Journal of Animal Research. 2016; 50 (6): 1013–017. https://doi.org/10.18805/ijar.9370
20. Albayrak H., Ozan E., Kadi H., Cavunt A., Tamer C., Tutuncu M. Molec- ular detection and seasonal distribution of lumpy skin disease virus in cattle breeds in Turkey. Medycyna Weterynaryjna. 2018; 74 (3): 175–178. https://doi.org/10.21521/mw.6081
21. Ince O. B., Türk T. Analyzing risk factors for lumpy skin disease by a geographic information system (GIS) in Turkey. Journal of the Hellenic Veterinary Medical Society. 2020; 70 (4): 1797–1804. https://dx.doi.org/10.12681/jhvms.22222
22. Ün H., Yumusak N., Özgünlük I., Yilmas R., Çabalar M. A lumpy skin disease case in the Southeast Turkey: A threat for Eurasia. Indian Jour- nal of Animal Research. 2019; 53(1): 129–135. https://doi.org/10.18805/ijar.B-732
23. Doğan F., Dağalp S. B., Ataseven V. S., Farzani T. A. The molecular detection of lumpy skin disease virus from infected cattle in Turkey. Journal of Applied Biological Sciences. 2016; 10 (2): 1–3. https://dergipark.org.tr/en/download/article-file/416194
24. Mat B., Arikan M. S., Akin A. C., Çevrimli M. B., Yonar H., Tekindal M. A. Determination of production losses related to lumpy skin disease among cattle in Turkey and analysis using SEIR epidemic model. BMC Veterinary Research. 2021; 17:300. https://doi.org/10.1186/s12917-021-02983-x
25. Jarullah B. A. Incidence of lumpy skin disease among Iraqi cattle in Waset Governorate, Iraq Republic. International Journal of Advanced Research. 2015; 3 (4): 936–939. https://www.journalijar.com/uploads/393_IJAR-5553.pdf
26. Isapour H., Sakha M., Varshovi H. R. The effect of Iranian capripoxvirus vaccine strains on neutralizing antibody titer in cattle. Iranian Journal of Veterinary Science and Technology. 2020; 12 (2): 77–82. https://doi.org/10.22067/veterinary.v12i2.84928
27. Sameea Yousefi P., Dalir-Naghadeh B., Mardani K., Jalilzadeh-Amin G. Phylogenetic analysis of the lumpy skin disease viruses in northwest of Iran. Tropical Animal Health and Production. 2018; 50 (8): 1851–1858. https://doi.org/10.1007/s11250-018-1634-3
28. Ghalyanchilangeroudi A., Ziafati Kafi Z., Rajeoni A., Ataii J., Sadri N., Hajizamani N., et al. Molecular detection and phylogenetic analysis of lumpy skin disease virus in Iran. Iranian Journal of Veterinary Medicine. 2021; 15 (2): 169–173. https://doi.org/10.22059/ijvm.2020.299359.1005071
29. Şevik M., Doğan M. Epidemiological and molecular studies on lumpy skin disease outbreaks in Turkey during 2014–2015. Transboundary and Emerging Diseases. 2017; 64 (4): 1268–1279. https://doi.org/10.1111/tbed.12501
30. Tageldin M. H., Wallace D. B., Gerdes G. H., Putterill J. F., Greyling R. R., Phosiwa M. N., et al. Lumpy skin disease of cattle: an emerging problem in the Sultanate of Oman. Tropical Animal Health and Production. 2014; 46 (1): 241–246. https://doi.org/10.1007/s11250-013-0483-3
31. Abutarbush S. M., Hananeh W. M., Ramadan W., Al Sheyab O. M., Alnajjar A. R., Al Zoubi I. G., et al. Adverse reactions to field vaccination against lumpy skin disease in Jordan. Transboundary and Emerging Diseases. 2016; 63 (2): e213–e219. https://doi.org/10.1111/tbed.12257
32. Kasem S., Saleh M., Qasim I., Hashim O., Alkarar A., Abu-Obeida A., et al. Outbreak investigation and molecular diagnosis of Lumpy skin disease among livestock in Saudi Arabia 2016. Transboundary and Emerging Diseases. 2018; 65 (2): e494–e500. https://doi.org/10.1111/tbed.12769
33. Tuppurainen E., Oura C. Lumpy skin disease: an African cattle disease getting closer to the EU. Veterinary Record. 2014; 175 (12): 300–301. https://doi.org/10.1136/vr.g5808
34. Lezaar Y., Manneh M., Apolloni A., Berrada J., Bouslikhane M. Transboundary livestock network in Africa: How circulate pathogens and where to act to prevent the epizootics spread? Epidemiology Open Journal. 2023; 8 (1): 1–19. https://www.researchgate.net/publication/376785686
35. Hasib F. M. Y., Islam M. S., Das T., Rana E. A., Uddin M. H., Bayzid M., et al. Lumpy skin disease outbreak in cattle population of Chattogram, Bangladesh. Veterinary Medicine and Science. 2021; 7 (5): 1616–1624. https://doi.org/10.1002/vms3.524
Yazid Khatib, Postgraduate Student, Department of Veterinary Medicine, Agrarian and Technological Institute
6 Miklukho-Maklaya str., Moscow 117198
Khatib Ya. Lumpy skin disease in the Middle East – historical and statistical data. Veterinary Science Today. 2025;14(1):24-31. https://doi.org/10.29326/2304-196X-2025-14-1-24-31
600901, Vladimir Oblast, Vladimir, microraion Yur’evets, ulitsa Gvardeyskaya, 6
FGBI “ARRIAH”
tel.: 8 (4922) 26-15-12, add. 22-27
E-mail: nikeshina@arriah.ru






























