



Contents
Scroll to:
 Yu. A. Vatnikov,
E. D. Sotnikova,
V. I. Kuznetsov,
A. A. Razumova,
I. V. Shchurov,
O. A. Petrukhina,
A. A. Rudenko
Yu. A. Vatnikov,
E. D. Sotnikova,
V. I. Kuznetsov,
A. A. Razumova,
I. V. Shchurov,
O. A. Petrukhina,
A. A. Rudenko https://doi.org/10.29326/2304-196X-2024-13-4-387-395
Scroll to:
Veterinary specialists have lately observed comorbidity of heart and kidney diseases known as cardiorenal syndrome. Cardiorenal syndrome is typically defined as dysfunction of a primarily intact kidney under the influence of a complex of pathogenetic damaging factors that arise against the background of an underlying cardiac disease. The purpose of the work is to study the biochemical profile of blood serum in cats with cardiorenal syndrome arising against the background of hypertrophic cardiomyopathy. The studies were carried out on 24 physiologically healthy (control) cats, 24 diseased cats with uncomplicated forms of pathology (first group) and 25 cats with hypertrophic cardiomyopathy complicated by cardiorenal syndrome (second group). It was shown that cardiorenal syndrome may occur as a complication of hypertrophic cardiomyopathy in animals. Biochemical tests in animals with feline cardiorenal syndrome verified cytolysis of cardiomyocytes (increased serum activity of lactate dehydrogenase by 2.69 times, creatine phosphokinase by 2.02 times, increased serum concentration of cardiac troponin by 5.20 times as compared to healthy animals), azotemia (increased concentration in serum creatinine by 2.72 times, urea by 2.94 times, symmetric dimethylarginine by 2.60 times and cystatin C by 1.90 times as compared to healthy animals), enhanced ketogenesis, systemic inflammatory process (increased serum concentration of C-reactive protein by 1.55 times as compared to healthy animals), hypercholesterolemia, oxidative stress (decrease in serum activity of superoxide dismutase by 1.63 times, catalase by 4.67 times and glutathione peroxidase by 1.71 times, increase in the concentration of malondialdehyde by 1.79 times, ceruloplasmin by 2.50 times and diene conjugates by 1.85 times as compared to healthy animals), electrolyte imbalance in the form of hyperkalemia, hyponatremia, hyperphosphatemia and hypomagnesemia. Biochemical indicators such as serum concentrations of creatinine, troponin I, cystatin C, symmetric dimethylarginine and C-reactive protein can be considered reliable diagnostic markers for the presence of cardiorenal syndrome.
Vatnikov Yu.A., Sotnikova E.D., Kuznetsov V.I., Razumova A.A., Shchurov I.V., Petrukhina O.A., Rudenko A.A. Serum biochemical profile in case of cardiorenal syndrome in cats with hypertrophic cardiomyopathy. Veterinary Science Today. 2024;13(4):387-395. https://doi.org/10.29326/2304-196X-2024-13-4-387-395
Circulatory and excretory organs are morphologically and functionally closely related [1-5]. Combined heart and kidney dysfunction has often been noted by veterinary practitioners as a fundamentally new supra-nosological concept which is referred to as cardiorenal syndrome [6-9]. It should be mentioned that the term “cardiorenal syndrome” is defined as a secondary kidney disorder occurring in the setting of the underlying heart failure [9]. Renocardial syndrome with cardiac dysfunction occurring against the background of the chronic kidney disease has also been described in the literature [6]. At the current stage of veterinary science development, many aspects of clinical manifestation, pathophysiology, methods of early diagnosis and highly effective treatment of cardiorenal syndrome in animals remain understudied. Generally, clinical symptoms appear in the late stages of pathology development [3]. Therefore, working out effective ways of predicting the cardiorenal syndrome development in pedigree animals is of particular relevance.
Hypertrophic cardiomyopathy (HCM) in domestic cats is frequently reported by veterinary practitioners. The risk of cardiorenal complications may increase in the setting of decompensated left ventricular heart failure in cats with HCM [10-12]. It should be stated that the basic pathobiochemical factors underlying the development and progression of cardiorenal syndrome in cats with HCM are not described in the scientific literature. Obviously, there is a high clinical demand for conducting large-scale studies on improvement of diagnostic and therapeutic methods, as well as giving a pathogenetic rationale for the use of nephroprotectors and cardioprotectors in cats with HCM.
The aim of the work was to study the serum biochemical profile in cats with cardiorenal syndrome occurring in the setting of HCM.
The study was conducted in the Department of Veterinary Medicine of the Peoples’ Friendship University of Russia named after Patrice Lumumba and on the basis of veterinary clinics in Moscow and the Moscow Oblast. Physiologically healthy (n = 24, control group) cats with HCM without cardiorenal complications (n = 24, group I), and animals with HCM complicated by cardiorenal syndrome (n = 25, group II) were used in the experiment.
The HCM diagnosis was verified comprehensively. Arterial tonometry was performed using petMAP graphic II device (Cardio Command, USA) according to the standard method [13]. Echocardiography and dopplerography were performed using Mindray DP-60 equipment (China) [14]. Electrocardiographic tests were performed using MIDAS-EK1T-04 device (Russia) [15]. A PCE-90Vet haemanalyser (High Technology Inc., USA) [16] and a SpotChem EZ SP-4430 biochemical analyzer (ARKRAY Factory Inc., Japan) [17] were also used. The level of azotemia (serum creatinine ≥ 200 μmol/L) was considered a reliable criterion for the presence of cardiorenal syndrome.
Blood was collected from the forearm saphenous vein of cats on an empty stomach in the morning hours and placed into vacuum tubes containing blood coagulation activator. Sodium, potassium, ionised calcium, phosphorus, magnesium, glucose, urea, creatinine, C-reactive protein, total protein, albumin, as well as serum activity of aspartate transaminase, alanine transaminase, creatine phosphokinase, lactate dehydrogenase in feline sera were determined according to generally accepted methods. The concentrations of ketone bodies in blood were estimated using a FreeStyle Optium Xceed ketometer (Abbott Diabetes Care Ltd, UK) [18]. The level of symmetric dimethylarginine and cystatin C in serum was tested with enzyme-linked immunosorbent assay. The functional condition of cardiomyocyte membranes was assessed by serum concentration of troponin I [11]. The intensity of lipid peroxidation processes and antioxidant system in blood serum of cats with cardiorenal syndrome was assessed using test kits of Randox Laboratories Ltd. (UK) according to the manufacturer’s instructions on a spectrophotometer UN2CO-WFT2100 (China).
Mann – Whitney and Kruskal – Wallis methods were used to statistically analyze the obtained numerical data in STATISTICA 7.0 [10]. The median (Me) and interquartile range (IQ) values were determined.
The Kruskal – Wallis test performed for cats with feline cardiorenal syndrome showed high values of the H criterion and a high level of statistical significance in terms of the following biochemical parameters typical of such a phenomenon as cytolysis: serum activity of asparagine and alanine aminotransferases, lactate dehydrogenase, creatine phosphokinase, troponin I concentration (Table 1).
Thus, there was a statistically significant increase in serum activity of alanine aminotransferase (1.17-fold; p < 0.001), asparagine aminotransferase (1.95-fold; p < 0.001), lactate dehydrogenase (1.51-fold; p < 0.001), creatine phosphokinase (1.61-fold; p < 0.001) and troponin I concentration (4.00-fold; p < 0.001) in cats with non-complicated HCM forms (group I) as compared with healthy cats. In the sera of cats with HCM complicated by cardiorenal syndrome (group II), as compared with healthy cats, there was a statistically significant increase in activity of alanine aminotransferase (1.23-fold; p < 0.001), asparagine aminotransferase (2.83-fold; p < 0.001), lactate dehydrogenase (2.69-fold; p < 0.001), creatine phosphokinase (2.02-fold; p < 0.001) and troponin I concentration (5.20-fold; p < 0.001). It should also be added that a statistically significant increase in serum activity of aspartate aminotransferase (1.45-fold; p < 0.001), lactate dehydrogenase (1.79-fold; p < 0.001), creatine phosphokinase (1.26-fold; p < 0.01) and serum concentrations of troponin I (1.30-fold; p < 0.01) was found in cats with HCM complicated by cardiorenal syndrome, as compared with diseased cats without such a complication.
Statistically significant changes in serum concentrations of urea, creatinine, symmetric dimethylarginine and cystatin C in cats during the development of cardiorenal syndrome were observed using Kruskal – Wallis test (Table 2).
It has been revealed that a statistically significant increase in serum concentrations of urea (1.63 times; p < 0.001), creatinine (1.27 times; p < 0.001), symmetric dimethylarginine (1.40 times; p < 0.001) was registered in animals with uncomplicated forms of HCM (group I) as compared with healthy ones. There was a statistically significant increase in serum concentrations of urea (2.94-fold; p < 0.001), creatinine (2.72-fold; p < 0.001), symmetric dimethylarginine (2.60-fold; p < 0.001) and cystatin C (1.90-fold; p < 0.001) in cats with HCM complicated by cardiorenal syndrome (group II), as compared with healthy animals. A statistically significant increase in serum concentrations of urea (1.80-fold; p < 0.001), creatinine (2.15-fold; p < 0.001), symmetric dimethylarginine (1.86-fold; p < 0.001) and cystatin C (1.81-fold; p < 0.001) was established in cats with HCM complicated by cardiorenal syndrome, as compared with the diseased cats without such a complication.
Statistically significant changes in the concentrations of ketone bodies, cholesterol, total protein and albumin in the sera of cats with cardiorenal syndrome were detected using the Kruskal – Wallis test.
The data in Table 3 show that a statistically significant increase in serum glucose concentrations (1.13-fold; p < 0.05) was registered in cats with uncomplicated forms of HCM (group I) as compared with healthy cats. A statistically significant increase in the serum concentrations of ketone bodies (8.50-fold; p < 0.001), cholesterol (1.67-fold; p < 0.001), and a decrease in the concentrations of total protein (1.06-fold; p < 0.05) and albumin (1.10-fold; p < 0.05) were noted in the sera of cats with HCM complicated by cardiorenal syndrome (group II), as compared with healthy cats. A statistically significant increase in serum concentrations of ketone bodies (7.08-fold; p < 0.001), cholesterol (1.62-fold; p < 0.001) was found in cats with HCM complicated by cardiorenal syndrome, as compared with diseased cats without such a complication.
Statistically significant changes in pathobiochemical parameters indicating oxidative stress were observed in cats with cardiorenal syndrome, using the Kruskal – Wallis method.
The numerical data presented in Table 4 show that a statistically significant increase in serum concentrations of malondialdehyde (1.63-fold; p < 0.001), diene conjugates (1.49-fold; p < 0.001), and a decrease in activity of superoxide dismutase (1.53-fold; p < 0.001), catalase (2.33-fold; p < 0.001), glutathione peroxidase (1.23-fold; p < 0.001) were observed in animals with uncomplicated forms of HCM (group I), as compared with healthy cats. A statistically significant increase in the serum concentrations of malondialdehyde (1.79-fold; p < 0.001), ceruloplasmin (2.50-fold; p < 0.001), diene conjugates (1.85-fold; p < 0.001) and simultaneous decrease of activity of superoxide dismutase (1.63-fold; p < 0.001), catalase (4.67-fold; p < 0.001), glutathione peroxidase (1.71-fold; p < 0.001) were observed in sera of cats with HCM complicated with cardiorenal syndrome (group II), as compared with healthy animals. A statistically significant increase in the serum concentrations of malondialdehyde (1.10-fold; p < 0.001), ceruloplasmin (2.14-fold; p < 0.001), diene conjugates (1.25-fold; p < 0.001), a decrease in activity of catalase (2.00-fold; p < 0.001), glutathione peroxidase (1.35-fold; p < 0.01), an increase in activity of glutathione reductase (1.36-fold; p < 0.01) were established in cats with complicated cardiorenal syndrome, as compared with diseased cats without such a complication.
The Kruskal – Wallis test revealed statistically significant changes in biochemical parameters of electrolyte metabolism in cats with cardiorenal syndrome (Table 5).
Table 1
Biochemical parameters of the syndrome of hepatocyte and cardiomyocyte cytolysis in cats with feline hypertrophic cardiomyopathy depending on cardiorenal complications
|
Parameter |
Animal groups |
Kruskal –Wallis criterion |
|||||
|
control (n = 24) |
I (n = 24) |
II (n = 25) |
|||||
|
Me |
IQ |
Me |
IQ |
Me |
IQ |
||
|
Creatine phosphokinase, |
207.00 |
183.00–227.00 |
333.50* |
279.50–360.00 |
419.00* # |
381.00–457.00 |
H = 49.40 р < 0.001 |
|
Aspartate aminotransferase, U/L |
31.50 |
29.50–34.00 |
61.50* |
52.00–70.50 |
89.00* ## |
66.00–108.00 |
H = 41.90 р < 0.001 |
|
Alanine aminotransferase, U/L |
53.50 |
51.50–55.50 |
62.50* |
58.00–64.50 |
66.00* |
59.00–73.00 |
H = 22.70 р < 0.001 |
|
Lactate dehydrogenase, |
132.50 |
105.00–158.00 |
200.00* |
152.00–230.00 |
357.00* ## |
299.00–402.00 |
H = 33.80 р < 0.001 |
|
Troponin I, |
0.10 |
0.08–0.11 |
0.40* |
0.30–0.45 |
0.52* # |
0.40–0.60 |
H = 41.60 р < 0.001 |
|
Me – median; IQ – interquartile range; *(p < 0.001) – reliability of the difference between the indicators of groups I, II # (p < 0.01), ## (p < 0.001) reliability of the difference between the indicators |
|||||||
Тable 2
Biochemical parameters of renal excretory function in cats with cardiorenal syndrome
|
Parameter |
Animal groups |
Kruskal –Wallis |
|||||
|
control (n = 24) |
I (n = 24) |
II (n = 25) |
|||||
|
Me |
IQ |
Me |
IQ |
Me |
IQ |
||
|
Urea, |
5.45 |
5.05–6.40 |
8.90* |
6.75–9.75 |
16.00* # |
14.80–17.10 |
H = 57.80 р < 0.001 |
|
Creatinine, |
106.50 |
93.00–136.50 |
135.00* |
121.00–147.00 |
290.00* # |
257.00–313.00 |
H = 50.70 р < 0.001 |
|
Symmetric dimethylarginine, µg/dL |
10.00 |
8.00–11.00 |
14.00* |
11.00–17.00 |
26.00* # |
24.00–30.00 |
H = 54.60 р < 0.001 |
|
Cystatin C, |
1.00 |
0.75–1.40 |
1.05 |
0.85–1.45 |
1.90* # |
1.40–2.20 |
H = 24.50 р < 0.001 |
|
Me – median; IQ – interquartile range; * (p < 0.001) – reliability of the difference between the indicators of groups I, II # (р < 0.001) reliability of the difference between the indicators |
|||||||
Table 3
Biochemical parameters characterizing protein, fat, carbohydrate metabolism in cats with cardiorenal syndrome
|
Parameter |
Animal groups |
Kruskal – Wallis criterion |
|||||
|
control (n = 24) |
I (n = 24) |
II (n = 25) |
|||||
|
Me |
IQ |
Me |
IQ |
Me |
IQ |
||
|
Glucose, |
4.85 |
4.50–5.60 |
5.50* |
4.95–5.90 |
5.10 |
4.60–5.50 |
H = 3.60 р < 0.50 |
|
Ketone bodies, |
0.10 |
0.03–0.14 |
0.12 |
0.00–0.18 |
0.85** # |
0.59–0.85 |
H = 36.60 р < 0.001 |
|
Cholesterol, |
3.35 |
2.80–4.45 |
3.45 |
3.00–4.00 |
5.60** # |
5.20–6.50 |
H = 39.30 р < 0.001 |
|
Triglycerides, |
0.70 |
0.70–0.85 |
0.90 |
0.50–1.10 |
0.70 |
0.60–0.80 |
H = 2.30 р < 0.50 |
|
Total protein, |
66.00 |
61.00–72.00 |
64.00 |
61.00–68.00 |
62.00* |
57.00–64.00 |
H = 7.90 р < 0.05 |
|
Albumin, |
33.00 |
29.50–36.50 |
31.50 |
30.50–36.00 |
30.00* |
28.00–32.00 |
H = 9.60 р < 0.01 |
|
Me – median; IQ – interquartile range; * (р < 0.05), ** (р < 0.001) – reliability of the difference between the indicators of groups I, II # (р < 0.001) – reliability of the difference between the indicators |
|||||||
Table 4
Oxidative stress in cats with hepatorenal syndrome
|
Parameter |
Animal groups |
Kruskal – Wallis criterion |
|||||
|
control (n = 24) |
I (n = 24) |
II (n = 25) |
|||||
|
Me |
IQ |
Me |
IQ |
Me |
IQ |
||
|
Malondialdehyde, |
2.80 |
2.60–3.05 |
4.55* |
4.05–4.95 |
5.00* ## |
4.80–5.20 |
H = 51.80 р < 0.001 |
|
Ceruloplasmin, |
0.60 |
0.40-0.70 |
0.70 |
0.50–1.20 |
1.50* ## |
1.30–1.90 |
H = 32.50 р < 0.001 |
|
Diene conjugates, U/mL |
2.05 |
1.55–2.35 |
3.05* |
2.70–3.55 |
3.80* ## |
3.60–4.00 |
H = 47.40 р < 0.001 |
|
Superoxide dismutase, |
50.50 |
40.50–65.00 |
33.00* |
30.50–35.50 |
31.00* |
23.00–35.00 |
H = 28.90 р < 0.001 |
|
Catalase, |
1.40 |
1.25–1.50 |
0.60* |
0.50–0.75 |
0.30* ## |
0.20–0.40 |
H = 59.70 р < 0.001 |
|
Glutathione reductase, |
1.35 |
1.10–1.75 |
1.10 |
0.80–1.45 |
1.50 # |
1.20–1.60 |
H = 7.20 р < 0.05 |
|
Glutathione peroxidase, U/mL |
2.90 |
2.60–3.60 |
2.30* |
2.00–2.65 |
1.70* # |
1.50–2.10 |
H = 38.30 р < 0.001 |
|
Me – median; IQ – interquartile range; * (p < 0.001) – reliability of the difference between the indicators of groups I, II # (p < 0.01), ## (p < 0.001) reliability of the difference between the indicators |
|||||||
Table 5
Electrolyte metabolism in cats with cardiorenal syndrome
|
Indicator |
Animal groups |
Kruskal –Wallis criterion |
|||||
|
Control (n = 24) |
I (n = 24) |
II (n = 25) |
|||||
|
Me |
IQ |
Me |
IQ |
Me |
IQ |
||
|
Sodium, |
155.00 |
151.50–158.50 |
149.00** |
146.00–152.50 |
148.00** |
143.00–154.00 |
H = 12.40 p < 0.01 |
|
Potassium, |
3.60 |
3.35–3.75 |
4.05** |
3.65–4.75 |
4.40*** |
3.80–5.50 |
H = 18.40 p < 0.001 |
|
Ionised calcium, |
9.52 |
8.95–9.40 |
9.20 |
8.75–9.80 |
10.30*** # |
9.90–10.60 |
H = 25.40 p < 0.001 |
|
Inorganic phosphorus, |
4.50 |
3.70–4.80 |
5.70* |
5.25–6.45 |
11.00*** # |
8.10–13.80 |
H = 41.10 p < 0.001 |
|
Magnesium, |
2.10 |
1.80–2.30 |
2.20 |
1.85–2.40 |
1.50*** # |
1.30–1.80 |
H = 20.50 p < 0.001 |
|
Me – median; IQ – interquartile range; * (p < 0.05), ** (p < 0.01), *** (p < 0.001) – reliability of the difference between the indicators of groups I, II # (p < 0.001) – reliability of the difference between the indicators of groups I and II animals |
|||||||
Hyponatremia, hyperkalemia and hyperphosphatemia occurred in cats with uncomplicated forms of HCM as compared to healthy animals. A trend for development of hyponatremia, hyperkalemia, hyperphosphatemia and hypomagnesemia was observed in sera of cats with HCM complicated by cardiorenal syndrome, as compared to healthy ones. It was established that insignificant hypercalcaemia, as well as significant hyperphosphatemia and hypomagnesemia were found in cats with HCM complicated by cardiorenal syndrome, as compared with diseased cats without such a complication.
The test results showing changes in C-reactive protein concentration in cats during the development of cardiorenal syndrome are presented in the figure.
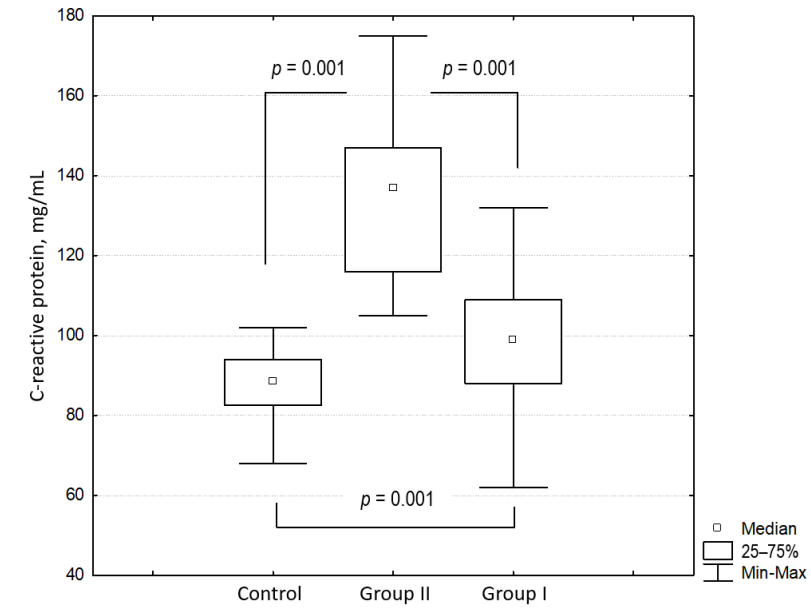
Fig. C-reactive protein concentration in cats with cardiorenal syndrome
Reliable changes in C-reactive protein concentration in sera of cats in different experimental groups were established (H = 50.50; p < 0.001; Kruskal – Wallis test). A statistically significant increase in C-reactive protein concentration in sera (1.15-fold; p < 0.001) was registered in animals with uncomplicated forms of HCM as compared to healthy animals. A statistically significant increase in C-reactive protein serum concentration (1.55-fold; p < 0.001) was registered in sera of cats with HCM complicated by cardiorenal syndrome as compared with healthy ones. It was also revealed that there is a statistically significant increase in C-reactive protein serum concentration in cats with HCM complicated by cardiorenal syndrome, as compared with diseased cats without such a complication.
Our study showed that the serum aminotransferase and lactate dehydrogenase activity is increased in cats with HCM. A significant increase in serum troponin concentration in HCM animals is indicative of damage to the cardiomyocyte cell membranes. Similar changes were previously described in the literature [1][10][12].
Azotemia developed in cats with cardiorenal syndrome occurring in the setting of HCM. It is obvious that this pathological process initially develops as prerenal azotemia, against the background of chronic circulatory insufficiency and, as a consequence, poor renal perfusion. However, as the pathology progresses, there is likely to be additional damage and death of nephrons, constituting a renal component in the pathogenesis of azotemia. Renal excretory dysfunction aggravates neuroendocrine shifts in the organism of diseased cats, which is also manifested by electrolyte metabolism disturbance (hyperkalemia, hyponatremia, hypomagnesemia, hyperphosphatemia). Obviously, the pathophysiological mechanism for a marked increase in serum concentration of inorganic phosphorus in animals with cardiorenal syndrome is secondary hyperparathyroidism, which often complicates the course of renal failure [18]. Uraemic toxins accumulating in the body during cardiorenal syndrome have an additional damaging effect on both cardiomyocytes and nephrons, which leads to further progression of the pathological condition.
The detection of ketosis in cats with cardiorenal syndrome was unexpected. It is obvious that there are profound changes in metabolism of animals with cardiorenal syndrome, that are manifested in adipose tissue mobilisation, increased protein and lipid catabolism, energy deficit. In such cases ketogenic amino acids and triglycerides may be the source of synthesis of ketone bodies. This phenomenon requires further large-scale studies. In our case, hypercholesterolemia, moderate hypoproteinemia and hypoalbuminemia were detected in diseased cats.
Systemic inflammation is the key pathogenetic link in the formation of cardiorenal syndrome in cats with HCM. Proinflammatory cytokines, which are produced during the development of the inflammatory response, have an additional damaging effect on cardiomyocytes and nephrons. High C-reactive protein serum concentrations can be considered as a marker of inflammation in cats with cardiorenal syndrome.
It is obvious that activation of the neurohumoral system against the background of circulatory failure and increased myocardial tissue oxygen demand can initiate cardiac cell apoptosis and fibrosis in cardiorenal syndrome. In this direction, further studies are required for morphological verification of the above pathological processes. Metabolic disorder in cardiomyocytes causes the development of oxidative stress, which increases the alterative effect on the myocardium.
Hypertrophic cardiomyopathy results in chronic circulatory failure in cats and may be complicated by cardiorenal syndrome. The activity of aspartate aminotransferase, lactate dehydrogenase, creatine phosphokinase, glutathione reductase significantly increases, and the concentrations of cardiac troponin, urea, creatinine, symmetric dimethylarginine, cystatin C, ketone bodies, cholesterol, malondialdehyde, ceruloplasmin, diene conjugates, potassium, calcium, phosphorus, C-reactive protein increase, the activity of superoxide dismutase, catalase and glutathione peroxidase, as well as the concentrations of total protein and albumin, sodium and magnesium decrease in the sera of cats with cardiorenal syndrome. Cardiorenal complications in cats with feline hypertrophic cardiomyopathy are characterised by the following biochemical syndromes: azotemia, cardiomyocyte cytolysis, electrolyte imbalance, systemic inflammatory reaction, oxidative stress.
1. Rudenko A. A. Evaluation of sleeping respiratory rate in cats with congestive heart failure: the degree of adherence to this test of animal owners and its impact on patient survival. Russian Veterinary Journal. 2018; (4): 9–14. https://doi.org/10.32416/article_5bd1c1f917fda5.38468318 (in Russ.)
2. Dudinskaya E. N. Cardiorenal metabolic health. Effective Pharmacotherapy. Endocrinology. 2023; 19 (52): 14–28. https://doi.org/10.33978/23073586-2023-19-52-14-28 (in Russ.)
3. Astrazhynski Ya. A., Kopats T. T. About the importance of cardiorenal syndrome in therapy. Scientific Medical Bulletin of Ugra. 2021; (Suppl.): 98–100. https://elibrary.ru/dynqtv (in Russ.)
4. Inatullaeva L. B., Vatnikov Yu. A., Vilkoviskiy I. F., Voronina Yu. Yu. Histological changes in kidneys with chronic kidney diseases in cats, associated with the deposition of amyloid. Veterinary, Zootechnics and Biotechnology. 2017; (5): 25–31. https://elibrary.ru/ytvint (in Russ.)
5. Phan V. T. Ph., Kontsevaya S. Yu. Osobennosti klinicheskogo proyavleniya serdechnoi nedostatochnosti u koshek, vyzvannoi kardiomiopatiei = Features of clinical manifestation of heart failure caused by cardiomyopathy in cats. Veterinarnaya khirurgiya: ot istoka k sovremennosti: materialy Mezhdunarodnoi nauchno-prakticheskoi konferentsii, posvyashchennoi 110-letiyu so dnya rozhdeniya professora, doktora veterinarnykh nauk G. S. Mastyko (Vitebsk, 3–5 noyabrya 2022 g.) = Veterinary surgery: from the origin to the present. Proceedings of the International Scientific and Practical Conference dedicated to the 110th anniversary of G. S. Mastyko, Professor, Doctor of Veterinary Science (Vitebsk, 3–5 November 2022). Vitebsk: Vitebsk State Academy of Veterinary Medicine; 2022; 191–193. https://elibrary.ru/zlrmnd (in Russ.)
6. Vatnikov Yu. A., Sotnikova E. D., Biakhova V. M., Petrukhina O. A., Matveev A. V., Rodionova N. Yu., Rudenko A. A. Features of the development of hepatocardial syndrome in dogs with dilated cardiomyopathy. Veterinariya. 2022; (10): 52–57. https://doi.org/10.30896/0042-4846.2022.25.10.5257 (in Russ.)
7. Rudenko A. A. Indices of specific cellular immunity in dogs with dilated cardiomyopathy. Veterinary, Zootechnics and Biotechnology. 2018; (6): 21–27. https://elibrary.ru/xvqwzv (in Russ.)
8. Sotnikova E. D., Petrukhina O. A., Byakhova V. M., Sibirtsev V. D. Features of the course of hepatocardial syndrome in cats with hypertrophic cardiomyopathy. RUDN Journal of Agronomy and Animal Industries. 2023; 18 (2): 264–272. https://doi.org/10.22363/2312-797X-2023-18-2-264-272
9. Shuteeva Yu. A., Maryushina T. O. Izuchenie narusheniya elektrolitnogo balansa u koshek s gipertroficheskoi kardiomiopatiei = Study of electrolyte imbalance in cats with hypertrophic cardiomyopathy. Molodezhnyi nauchnyi forum: estestvennye i meditsinskie nauki. 2017; (4): 167–171. https://elibrary.ru/ylixqh (in Russ.)
10. Khokhlova L. N., Kurkina N. V. Vyyavlenie kardiorenalnogo sindroma u bol’nykh s arterial’noi gipertenziei = Identifi ation of cardiorenal syndrome in patients with arterial hypertension. Aktual’nye problemy sovremennoi nauki v 21 veke: materialy XII Mezhdunarodnoi nauchnoprakticheskoi konferentsii (Makhachkala, 25 dekabrya 2016 g.) = Current issues of modern science in the 21st century: proceedings of the XII International Scientific and Practical Conference (Makhachkala, 25 December 2016). Makhachkala: Approbation; 2016; 167–168. https://elibrary.ru/xvbbvr (in Russ.)
11. Karpenko L. Yu., Kozitcyna A. I., Bakhta A. A., Polistovskaya P. A. Prognostic criteria for assessing of hypertrophic cardiomyopathy in cats. Legal Regulation in Veterinary Medicine. 2022; (1): 44–46. https://doi.org/10.52419/issn2782-6252.2022.1.44 (in Russ.)
12. Phan V. T. Ph., Kontsevaya S. Yu., Orlov S. M. Retrospective evaluation of cardiomyophaty disease in 27 cats with heart failure disease. Actual Questions of Veterinary Biology. 2022; (4): 26–32. https://doi.org/10.24412/20745036-2022-4-26-32 (in Russ.)
13. Junusbekova G. A., Dzhusipov A. K. Vedushchie patogeneticheskie mekhanizmy razvitiya kardiorenal’nogo porazheniya pri arterial’noi gipertonii = Leading pathogenetic mechanisms of cardiorenal damage development in arterial hypertension. I Evraziiskii kongress kardiologov. I Natsional’nyi kongress kardiologov Kazakhstana: sbornik tezisov (Astana, 20–21 oktyabrya 2009 g.). = I Eurasian Congress of Cardiologists. I National Congress of Cardiologists of Kazakhstan: collection of abstracts (Astana, 20–21 October 2009). Moscow: InterMedservis; 2009; 94. https://elibrary.ru/ynefjb (in Russ.)
14. Dzugkoeva F. S., Gatagonova T. M., Lolaeva A. T., Dzugkoev S. G., Brtsieva Z. S. Kardiorenal’nye mikrotsirkulyatornye narusheniya pri patologii vistseral’nykh organov i ikh patogeneticheskaya korrektsiya = Cardiorenal microcirculatory disorders in pathology of visceral organs and their pathogenetic correction. Fundamental Research. 2009; (7-S): 46–47. https://elibrary.ru/kxqied (in Russ.)
15. Kostylev V. A., Goncharova A. V. Ekhokardiograficheskaya kharakteristika gipertroficheskoi kardiomiopatii koshek porody mein-kun = Echocardiographic characteristics of hypertrophic cardiomyopathy in Maine Coon cats. Aktual’nye problemy veterinarnoi meditsiny, zootekhnii, biotekhnologii i ekspertizy syr’ya i produktov zhivotnogo proiskhozhdeniya: sbornik trudov nauchno-prakticheskoi konferentsii (Moskva, 8 noyabrya 2022 g.) = Current issues of veterinary medicine, zootechnics, biotechnology and veterinary and sanitary examination of raw materials and products of animal origin: proceedings of the Scientific and Practical Conference (Moscow, 8 November 2022). Ed. by S. V. Pozyabin, L. A. Gnezdilova. Moscow: Agricultural technologies; 2022; 100–102. https://elibrary.ru/pvedob (in Russ.)
16. Kryukovskaya G. M., Kryukovsky R. A., Lutsay V. I., Boyunchan N. R. Fazovo-kontrastnaya mikroskopiya dlya otsenki eritrotsitov v posttravmaticheskom periode u zhivotnykh posle krovopoter’= Phase-contrast microscopy for erythrocyte assessment in animals in the post-traumatic period after blood loss. Razrabotka innovatsionnykh instrumental’nykh metodov issledovaniya vnutrennikh boleznei zhivotnykh: sbornik trudov II Nauchnoi konferentsii (Moskva, 12–13 fevralya 2015 g.) = Development of innovative instrumental methods for studying internal animal diseases: proceedings of the II Scientific Conference (Moscow, 12–13 February 2015). Moscow: Moscow State Univetsity of Food Production; 2015; 53–57. https://elibrary.ru/untlrj (in Russ.)
17. Soldatenko N. V. Features of cardiorenal disorders and the possibilities of their adequate correction in patients with arterial hypertension and primary subclinical hypothyroidism: Author’s Thesis for Degree of Cand. Sci. (Medicine). Stavropol; 2014. 157 p. (in Russ.)
18. Filippov Yu. I., Pozyabin S. V., Belogurov V. V. Dietoterapiya koshek s khronicheskoi pochechnoi nedostatochnost’yu = Diet therapy for cats with chronic renal failure. VetPharma. 2014; (5): 28–30. https://elibrary.ru/sxcqrn (in Russ.)
Yury A. Vatnikov, Dr. Sci. (Veterinary Medicine), Professor, Director of Department of Veterinary Medicine
6 Miklukho-Maklaya str., Moscow 117198
Elena D. Sotnikova, Cand. Sci. (Biology), Associate Professor of Department of Veterinary Medicine
6 Miklukho-Maklaya str., Moscow 117198
Vladimir I. Kuznetsov, Dr. Sci. (Medicine), Professor of Department of General Medical Practice
6 Miklukho-Maklaya str., Moscow 117198
Alisa A. Razumova, Cand. Sci. (Biology), Head of the Department for Research Coordination
Yur’evets, Vladimir 600901, Russia
Igor V. Shchurov, Cand. Sci. (Veterinary Medicine), Head of Center for Veterinary Innovative Medicine
6 Miklukho-Maklaya str., Moscow 117198
Olesia A. Petrukhina, Cand. Sci. (Veterinary Medicine), Assistant of Department of Veterinary Medicine
6 Miklukho-Maklaya str., Moscow 117198
Andrey A. Rudenko, Dr. Sci. (Veterinary Medicine), Associate Professor, Professor of Department of Veterinary Medicine
11 Volokolamskoe highway, Moscow 125080, Russia
Vatnikov Yu.A., Sotnikova E.D., Kuznetsov V.I., Razumova A.A., Shchurov I.V., Petrukhina O.A., Rudenko A.A. Serum biochemical profile in case of cardiorenal syndrome in cats with hypertrophic cardiomyopathy. Veterinary Science Today. 2024;13(4):387-395. https://doi.org/10.29326/2304-196X-2024-13-4-387-395
600901, Vladimir Oblast, Vladimir, microraion Yur’evets, ulitsa Gvardeyskaya, 6
FGBI “ARRIAH”
tel.: 8 (4922) 26-15-12, add. 22-27
E-mail: nikeshina@arriah.ru






























